Many men with benign prostatic hyperplasia experience urinary problems related to the condition. As the prostate enlarges, the gland places increasing pressure on the urethra, often resulting in difficulty beginning or ending urination, an inability to completely empty the bladder, decreased urine flow, and frequent urination. In the most severe cases, complete blockage of the urethra occurs, which may lead to kidney damage.
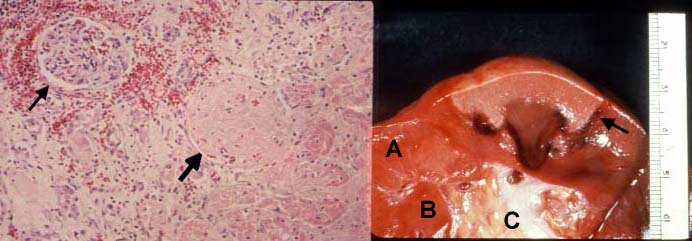
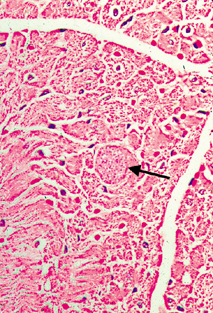
From microscopyu.com Benign Prostatic Hyperplasia at 20x Magnification :

Part of the male reproductive system, the prostate gland produces and stores seminal fluids, releasing them into the urethra when semen emission occurs. The gland is located directly below the bladder and surrounds the upper part of the urethra. During adolescence the gland usually matures and reaches a size comparable to that of a walnut. The dimensions of the gland generally remain unchanged for several decades, but in most older men, the prostate begins to enlarge as the size of its cells increases, a process commonly referred to as benign prostatic hyperplasia (BPH) or hypertrophy. According to recent estimates, more than 50 percent of men between the ages of 50 and 60 experience benign prostatic hyperplasia, and over 90 percent of those 70 to 90 years old have developed the condition. Researchers do not yet completely understand the cause of this physiological change, but it is widely thought that elevated levels of the female sex hormone estradiol and increased manufacture of dihydrotestosterone, a derivative of the male sex hormone testosterone, contribute to the condition.
Benign Prostatic Hyperplasia at 4x Magnification :

Men with only mild symptoms of benign prostatic hyperplasia may elect not to undergo any treatment or to simply take a wait-and-see attitude, visiting the doctor regularly for monitoring until signs suggest a more active approach is needed. For those who seek treatment, a number of options are available. For example, drugs such as alpha blockers and finasteride may be used alone or in conjunction with one another to relax prostatic smooth muscle and decrease the size of the prostate gland. Individuals that are not responsive to the typical medications, however, may require a more invasive form of treatment, such as balloon dilation of the urethra or any of several different surgical techniques, including transurethral incision of the prostate (TUIP), transurethral resection of the prostate (TURP), or open prostatectomy. The various treatments for benign prostatic hyperplasia are associated with a number of risks and side effects, which can include serious conditions like incontinence and impotence.