
health, acne, acne vulgaris, cancer,
Showing posts with label GIT SURGERY. Show all posts
Showing posts with label GIT SURGERY. Show all posts
Tuesday, 19 July 2011
Saturday, 7 May 2011
Dumping syndrome after peptic ulcer surgery
A 44-year-old man with a history of peptic ulcer surgery presents with palpitations, tachycardia, lightheadedness, and diaphoresis after eating a meal. The symptoms typically begin 30 min after eating.Which of the following is the most likely diagnosis?

Some patients with a history of ulcer surgery experience the dumping syndrome 30 min after eating. They present with palpitations, tachycardia, lightheadedness, and diaphoresis after eating a meal due to the rapid emptying of hyperosmolar gastric contents into the small intestine.
Dumping syndrome is also called rapid gastric emptying which occurs when the undigested food bypass the stomach and transported or "dumped" into the small intestine too rapidly.
- a.Malabsorption
- b.Peptic ulcer recurrence
- c.Gastric carcinoma
- d.Gastritis
- e.Dumping syndrome
- f.Esophagitis
The answer is (e).

Some patients with a history of ulcer surgery experience the dumping syndrome 30 min after eating. They present with palpitations, tachycardia, lightheadedness, and diaphoresis after eating a meal due to the rapid emptying of hyperosmolar gastric contents into the small intestine.
Dumping syndrome is also called rapid gastric emptying which occurs when the undigested food bypass the stomach and transported or "dumped" into the small intestine too rapidly.
Thursday, 17 March 2011
Notes on gallbladder stones
The photo below shows multiple faceted gallstones that can be composed of either cholesterol, bile pigments or a mixture of the two.
-Pigment stones are often small and occur in patients with either congenital or acquired haemolytic states (5%).
-Cholesterol stones are often large and solitary (15%).
The stones shown are mixed stones and account for approximately 80% of all gallstones.
"Mixed stones are probably a variant of cholesterol stones"
 This picture shows a collection of gallstones removed from a gall bladder during a cholecystectomy. Gallstones are more common in females than males. And there prevalence increases with age and diabetes mellitus, obesity, ileal disease and certain drugs (e.g. Clofibrate) appear to be important in the aetiology.
This picture shows a collection of gallstones removed from a gall bladder during a cholecystectomy. Gallstones are more common in females than males. And there prevalence increases with age and diabetes mellitus, obesity, ileal disease and certain drugs (e.g. Clofibrate) appear to be important in the aetiology.
Only 10% of gallstones are symptomatic.Also about 10% of gallstones are radio-opaque and visible on a plain abdominal film.
-Pigment stones are often small and occur in patients with either congenital or acquired haemolytic states (5%).
-Cholesterol stones are often large and solitary (15%).
The stones shown are mixed stones and account for approximately 80% of all gallstones.
"Mixed stones are probably a variant of cholesterol stones"
Pathophysiology:
Cholesterol stones result from a change in solubility of bile constituents- Bile acids act as a detergent keeping cholesterol in solution
- Bile acids, lecithin and cholesterol result in the formation of micelles
- Bile is often supersaturated with cholesterol
- This favours the formation of cholesterol microcrystals
- Biliary infection, stasis and changes in gallbladder function can precipitate stone formation

Only 10% of gallstones are symptomatic.Also about 10% of gallstones are radio-opaque and visible on a plain abdominal film.
Tuesday, 15 March 2011
Barrett's esophagus
The Key word :
BARRett's = Becomes Adenocarcinoma, Results from Reflux.
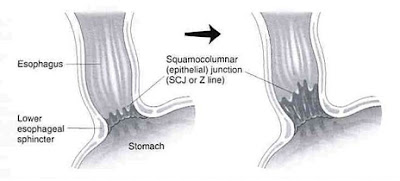 Barrett's esophagus is a Glandular metaplasia ,or replacement of non keratinized (stratified) squamous epithelium with intestinal (columnar) epithelium in the distal esophagus as a serious uncommon complication of chronic acid reflux or GERD (gastroesophageal reflux disease) .
Barrett's esophagus is a Glandular metaplasia ,or replacement of non keratinized (stratified) squamous epithelium with intestinal (columnar) epithelium in the distal esophagus as a serious uncommon complication of chronic acid reflux or GERD (gastroesophageal reflux disease) .
 By endoscope :
By endoscope :
the color and composition of the tissue lining the lower esophagus change. Instead of pink, the tissue turns a salmon color.
Under a microscope, the tissue resembles that of the small intestine "metaplasia".
This Metaplasia is brought on by repeated and long-term exposure to stomach acid and is associated with an increased risk of esophageal cancer.

BARRett's = Becomes Adenocarcinoma, Results from Reflux.

 By endoscope :
By endoscope :the color and composition of the tissue lining the lower esophagus change. Instead of pink, the tissue turns a salmon color.
Under a microscope, the tissue resembles that of the small intestine "metaplasia".
This Metaplasia is brought on by repeated and long-term exposure to stomach acid and is associated with an increased risk of esophageal cancer.

Wednesday, 2 March 2011
Saturday, 26 February 2011
Friday, 11 February 2011
Placement Percutaneous Endoscopic Gastrostomy tube
Placement of a Flocare PEG tube (Percutaneous Endoscopic Gastrostomy tube) in a patient who previously was fed via a naso-gastric tube.
The video shows detailed instructions for placement, immediate care and long-term care of the PEG tube.
The video shows detailed instructions for placement, immediate care and long-term care of the PEG tube.
Tuesday, 8 February 2011
Tuesday, 28 December 2010
Sunday, 26 December 2010
Thursday, 23 December 2010
Thursday, 9 December 2010
Laparoscopic Gastric Banding with Autonomy Needle Holder
Laparoscopic Gastric Banding with Autonomy Articulating Needle Holder by Dr. Dmitry Nepomnayshy.
Diagrams for Surgical Procedures of Chronic Pancreatitis
The selection of the operative procedure often depends on the surgeon's expertise and individual preference. There is some criteria that usually favor one type of surgery over another. When the pancreatic duct in the body or tail is dilated beyond 6 mm, the Puestow procedure is usually the most effective surgery . When disease occurs predominantly in the head, Frey's procedure is used. When there is a focal mass in the head without significant duct dilation, the Whipple procedure is most frequently used. Increasingly, Beger's procedure, which preserves the duodenum, is used as an alternative.




1-Whipple Procedure:
The most common pancreatic resection surgery is the Whipple procedure, which is performed for chronic pancreatitis with ductal strictures or amorphous inflammatory mass in the head for which distinction from cancer cannot be made preoperatively. However, many specialist pancreatic surgeons no longer consider this to be the most appropriate surgery for chronic pancreatitis.
Diagram of pylorus-preserving Whipple procedure. Classic Whipple procedure is shown in inset: It entails radical dissection of pancreatic head, adjacent nodes, right half of omentum, gall bladder, common bile duct, and most or all of duodenum followed by gastrojejunostomy/duodenojejunostomy (green arrow), pancreaticojejunostomy (blue arrow), and hepaticojejunostomy (red arrow). (Courtesy of the Office of Visual Media, Indiana University)
2-Beger's Procedure :
Beger's procedure is a less radical surgery with resection of the pancreatic head and preservation of the duodenum . After Beger's surgery, pain relief is seen in up to 85% of patients at 5-year follow-up , but the postoperative morbidity rate is 20%. A randomized study comparing Beger's and Whipple procedures showed similar results at 6 months except for better pain tolerance and glucose control in those treated with Beger's surgery.
Diagram of Beger's procedure. Pancreatic body and most of head have been resected. Sleeve of pancreas is left with duodenum to preserve blood supply for latter. This procedure is technically harder to perform than Whipple procedure. Note pancreaticojejunostomy (red arrows) at two sites of Roux limb (green arrow).
3-Puestow Procedure :
The Puestow procedure is a side-to-side longitudinal pancreaticojejunostomy that drains the pancreatic duct directly into a loop of jejunum . This procedure is best performed if the main pancreatic duct is significantly dilated, usually wider than 6 mm.
Diagram of Puestow procedure. Pancreas is filleted to expose main duct from neck to tail and ductal calculi are removed. Roux loop is anastomosed to "capsule" of pancreas with direct drainage of main and secondary pancreatic ducts into jejunum over 8- to 10-cm segment. Loop (arrows) lies anterior to pancreas.
4-Frey's Procedure :
Frey's procedure is a recently popularized procedure that combines partial resection of the pancreatic head with a longitudinal jejunostomy . The morbidity rate of Frey's procedure is approximately 9-22% , well below that of the Whipple procedure performed for chronic pancreatitis, for which the complication rate is 30-40% . Frey's procedure is contraindicated in the presence of duodenal or biliary stricture.
Diagram of pancreas after Frey's procedure. Head of pancreas is cored out (blue arrow) and pancreaticojejunostomy is created via Roux loop (green arrows). Procedure is best performed in patients with duct dilation of head and body.
Pelvic Spleen

A healthy, 23-year-old, nulliparous woman presented with lower abdominal pain, which she reported having had intermittently for the previous year. She had no other symptoms of gastrointestinal distress. A peripheral-blood smear showed no Howell–Jolly bodies.
Physical examination revealed a palpable mass in the suprapubic region. Abdominal ultrasonography revealed displacement of the spleen from its normal position and a homogeneous soft-tissue mass (measuring 11.0 by 9.3 by 4.2 cm) in the pelvis. Imaging of the liver and spleen after injection of technetium-99m sulfur colloid (Panel A) revealed a normal liver and a well-defined area showing abnormal accumulation of radiotracer (arrow) in the lower abdomen.
Multislice computed tomography, with three-dimensional reconstruction of a coronal image (Panel B), revealed the position of the spleen in the pelvis (black arrow), with torsion of the elongated pedicle (white arrow).
Wandering spleen, or pelvic spleen, is an uncommon condition associated with laxity or malformation of the suspensory ligaments of the spleen. Splenic torsion and infarction are potential complications. The principal therapeutic options are splenopexy and splenectomy. After discussion of treatment options, the patient declined surgical intervention and has continued to do so in follow-up over the past 3 years.
Monday, 6 December 2010
Differential Diagnosis of bile duct dilatation
Whenever there is bile duct dilatation, the first priority is to look for obstruction.

Obstruction
If there is an obstruction, we first look for gallstones in the bile duct. If there are no gallstones involved, we then look for strictures.
The differential diagnosis for a stricture is based on the location.
* A distal stricture is most likely the result of a distal cholangiocarcinoma, pancreatic carcinoma or pancreatitis.
* A stricture within the liver is likely due to gallbladder carcinoma or inflammatory strictures like PSC (Primary Sclerosing Cholangitis) or AIDS cholangiopathy.
* Metastatic disease can occur anywhere within the bilairy system.
No Obstruction
Once we have excluded obstruction, we have to think about nonobstructive biliary diseases like:
* Caroli disease
* Choledochal cyst
* Recurrent pyogenic cholangitis
* Primary sclerosing cholangitis

Obstruction
If there is an obstruction, we first look for gallstones in the bile duct. If there are no gallstones involved, we then look for strictures.
The differential diagnosis for a stricture is based on the location.
* A distal stricture is most likely the result of a distal cholangiocarcinoma, pancreatic carcinoma or pancreatitis.
* A stricture within the liver is likely due to gallbladder carcinoma or inflammatory strictures like PSC (Primary Sclerosing Cholangitis) or AIDS cholangiopathy.
* Metastatic disease can occur anywhere within the bilairy system.
No Obstruction
Once we have excluded obstruction, we have to think about nonobstructive biliary diseases like:
* Caroli disease
* Choledochal cyst
* Recurrent pyogenic cholangitis
* Primary sclerosing cholangitis
Tuesday, 30 November 2010
Appearance of lye strictures in X-ray

-What is the most likely diagnosis in the patient shown below?
a. Esophageal varices
b. Esophageal carcinoma
c. Reflux esophagitis
d. Lye stricture
e. Fibrovascular polyp
THE RIGHT ANSEWR : .d
There is very long segment of smoothly narrowed esophagus from just below the level of the clavicles to the EG junction. This appearance is characteristic of a stricture caused by the ingestion of a caustic material such as lye. Lye, which became component of some drain cleaners in the late ?60s, is so highly toxic that only a few drops can cause this full-thickness liquefaction necrosis of the esophagus. The acute ulcerative phase is invariably followed in several weeks by this fibrotic stage. There is a significantly higher incidence of carcinoma of the esophagus in patients with lye strictures than in the normal population.
Sunday, 28 November 2010
Ileocecal Intussusception

Physical examination showed moderate abdominal distention. Computed tomographic scans of his abdomen revealed an ileocecal intussusception (Panel A, arrow) with a pathologic mass, 2.5 cm in diameter, at the apex, also known as the lead point (Panel B, arrow). Diagnostic laparoscopy was performed, and the diagnosis of intussusception was confirmed.
Laparoscopically assisted ileocecal resection with primary anastomosis was performed. Gross inspection of the specimen showed a pedunculated lipoma within the terminal ileum. The patient had a rapid recovery, with complete resolution of his symptoms.
Saturday, 27 November 2010
Friday, 26 November 2010
Gastric diverticulum PIC

Upper gastrointestinal endoscopic scan showing a diverticulum (arrow) in the fundus of the stomach.
Gastric diverticula are uncommon.with equal distribution among men and women, and can be congenital or acquired.Areas of weakness caused by splitting of the longitudinal muscle fibres, an absence of peritoneal membrane and perforating arterioles may predispose to the formation of a diverticulum.Patients with gastric diverticula are often asymptomatic, although they may present with dyspepsia, vomiting and abdominal pain. Complications such as ulceration, perforation, hemorrhage, torsion and malignancy are uncommon. The condition is diagnosed incidentally by radiologic or endoscopic examination. There is no specific treatment required for an asymptomatic diverticulum.
Surgical resection is recommended when the diverticulum is large, symptomatic or complicated by bleeding, perforation or malignancy. Both open and laparoscopic resection yield good results. Perioperative gastroscopy can help locate the diverticulum in difficult situations.
WATCH THE VIDEO
Subscribe to:
Posts (Atom)